Common Badminton Injuries & How to Prevent Them: Shoulder, Elbow, Knee, Ankle
7 June 2026 · Badminton Fans
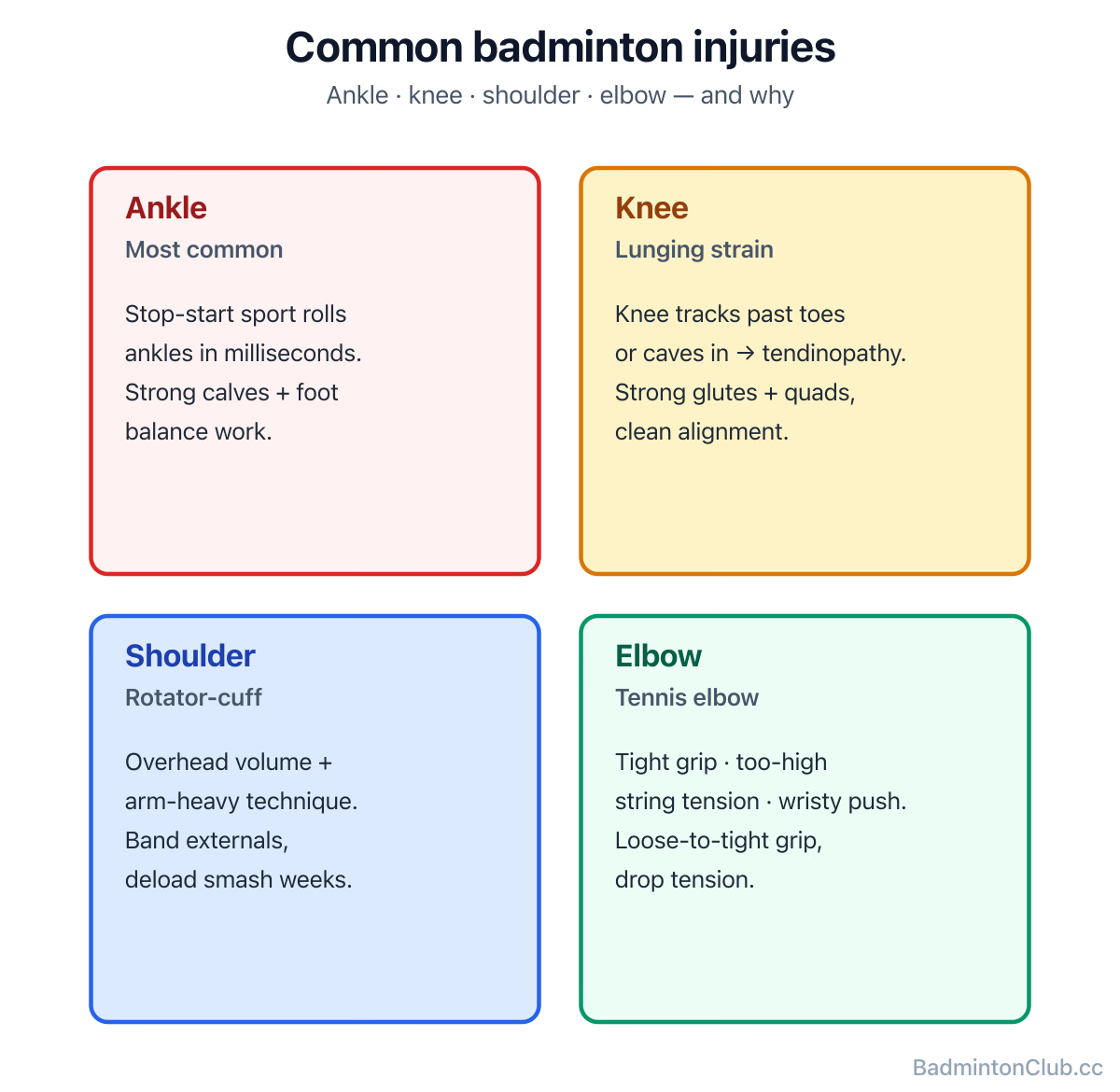
The four most common badminton injuries are: rolled or sprained ankles (often the most frequent), knee strain from lunging and landing, rotator-cuff and shoulder overuse from overhead strokes, and lateral epicondylitis ("tennis elbow") from gripping too tight or playing with poor wrist-and-forearm mechanics — all of them largely preventable with a proper warm-up, technique work, and targeted strengthening. This guide isn't medical advice; persistent pain means see a physio.
Ankle sprains — the most common
Why: badminton is a stop-start sport with sudden lunges, lateral pushes and landings; a poorly placed foot rolls the ankle in milliseconds. Prevention: strong calves and intrinsic foot muscles, single-leg balance work (2–3 min/day), proper non-marking court shoes (see Badminton Shoes (separate guide)) replaced before they wear, and a real warm-up. Recovery if it happens: standard RICE in the first 48 hours (rest, ice, compression, elevation), then progressive loading. Taping the ankle can help during return-to-play — a basic figure-of-eight or stirrup with athletic tape supports the lateral ligaments; if you're routinely needing tape to play, you need rehab, not more tape. See a physio for any sprain that doesn't resolve in 7–10 days.
Knee pain — usually from lunging
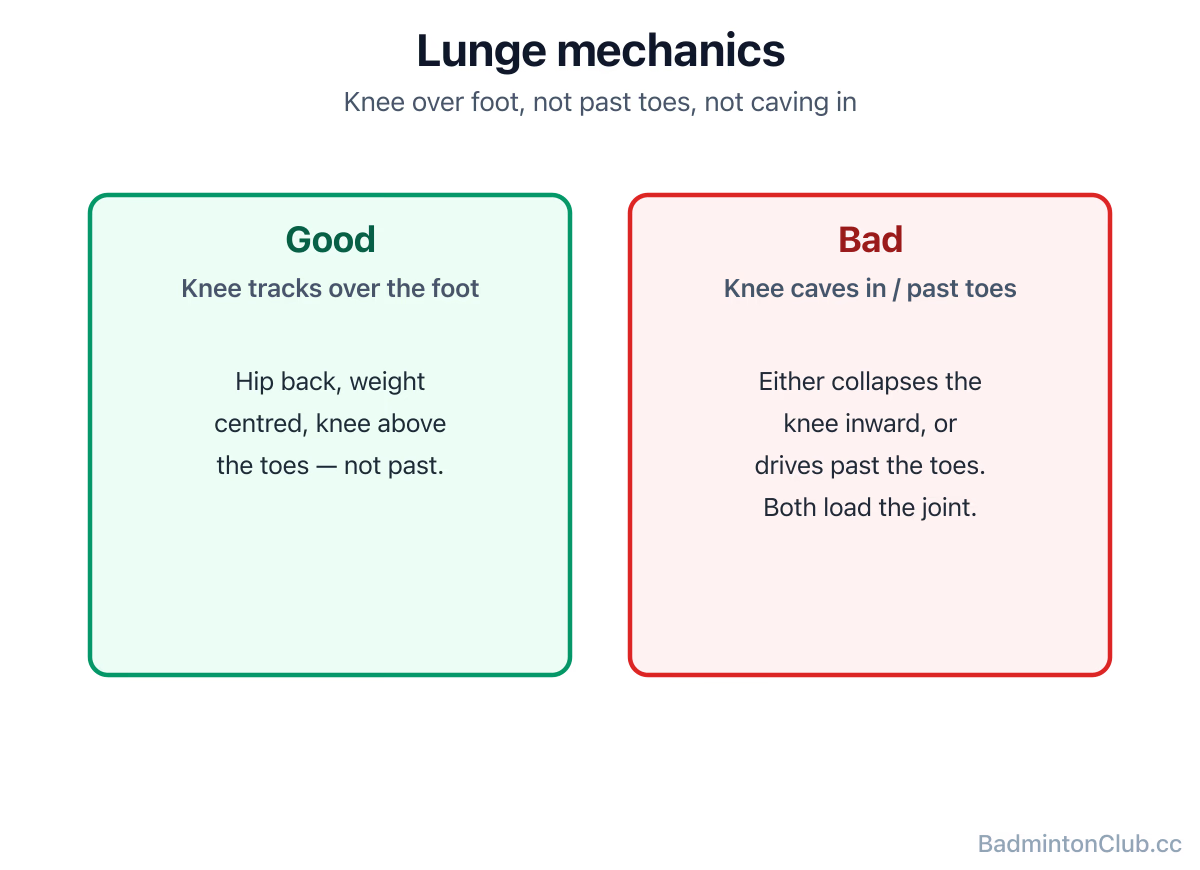
Why: badminton lunges load the front knee heavily; if the knee tracks past the toes or caves inward, the patellar tendon and the soft tissues around the knee complain. Repeated jumping with a hard landing adds to it. Prevention: strong quads, glutes and hamstrings (see Strength Training), good lunge mechanics (knee over the foot, not past the toes, hips back), and quality landing mechanics out of jumps. Warning sign: sharp pain (not just stiffness) during a lunge or going down stairs — back off and see a physio. Pushing through knee pain is how minor patellar issues become long-term tendinopathy.
Shoulder & rotator-cuff overuse
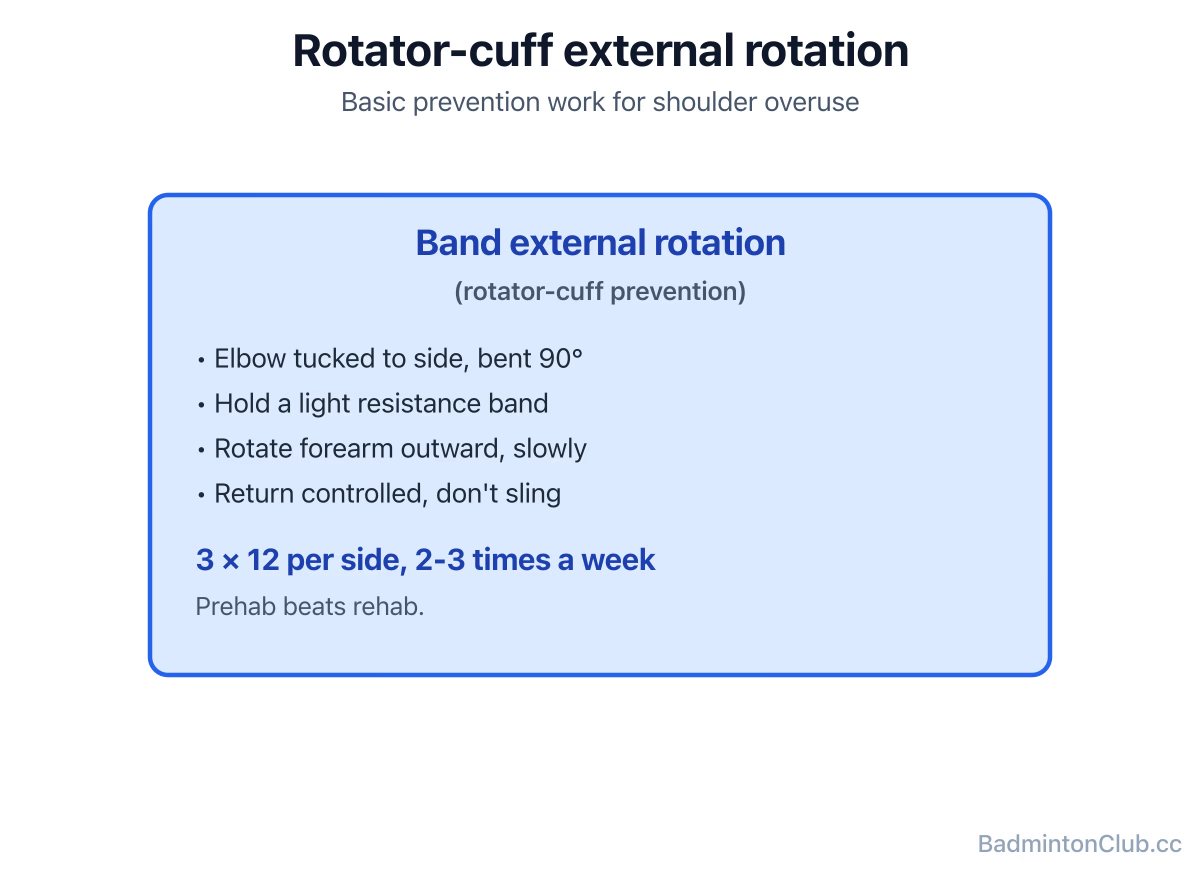
Why: the overhead smash and clear repeatedly load the small stabilising muscles of the shoulder (the rotator cuff). High volume + poor technique (too much arm, not enough kinetic chain — see How to smash harder) is the classic recipe for chronic shoulder pain. Prevention: rotator-cuff strengthening (external rotations with a light band, 3 × 12, 2–3 times/week), thoracic spine mobility (the upper back), and deloading smash volume in heavy training weeks. A "smash-only" session two days running is asking for trouble. Treatment of mild overuse: reduce overhead volume, add band work, see a physio if it persists more than 2 weeks.
Tennis elbow (lateral epicondylitis)
Why: despite the name, racket-sport elbow pain comes mostly from gripping too tight, using a racket with too-stiff strings at too-high tension, or hitting the shuttle with a wristy push instead of a relaxed-to-fast forearm snap. Prevention: loose-to-tight grip (squeeze only at impact), sensible string tension (most club players over-tension — see String Tension Guide (separate guide)), and forearm strengthening (light pronation/supination, eccentric wrist extensions). Bracing: an epicondylitis strap can offload the tendon during return-to-play, but it doesn't fix the cause. If your elbow is sore, change your technique and tension first, not your brace.
A general prevention checklist
- Always warm up dynamically (see Warm-up & flexibility).
- Build strong, stable ankles and knees with targeted single-leg work.
- Lift twice a week — strength is injury insurance.
- Don't pile high-volume overhead days back-to-back.
- Replace shoes before they wear flat.
- Listen to pain. Stiffness is normal; sharp pain isn't. See a physio early; small problems caught early are days off, ignored ones are months.
What this looks like on a club night
The injuries that take people out of badminton aren't dramatic — they're the slow ones. The recurring ankle that keeps "going" because no one ever rehabbed it properly. The shoulder that's been dull-aching for a year and finally gives out mid-smash. The elbow that's been quietly tightening because the strings are at 28 lbs and the grip is white-knuckled. A frank opinion: most club injuries are technique and habit problems, not bad luck. Fix the habits — warm up, lift, replace shoes, loosen the grip — and you'll keep playing for years longer. If your club uses BadmintonClub.cc, the player-status field is a quiet, useful place to flag "returning from ankle" or "shoulder load light this week" so partners and rotation organisers don't accidentally push you into the deep end of the box.
This is not medical advice. For any persistent or sharp pain, see a sports physiotherapist.
FAQ
- Q: What's the most common badminton injury? Rolled or sprained ankles, followed by knee strain from lunging, shoulder/rotator-cuff overuse, and tennis elbow.
- Q: Why does my shoulder hurt after playing badminton? Most often rotator-cuff overuse from high overhead volume and arm-heavy technique — add band external rotations, reduce smash volume in heavy weeks, and see a physio if pain persists more than 2 weeks.
- Q: How do I protect my knees during lunges? Keep the front knee tracking over the foot (not past the toes, not caving in), build strong quads and glutes, and never lunge cold — always warm up first.
- Q: How do I tape my ankle for badminton? A basic figure-of-eight or stirrup with athletic tape supports the lateral ligaments during return-to-play, but recurring tape use means you need rehab, not more tape.
- Q: How do I treat tennis elbow from badminton? Loosen your grip, drop string tension if it's high, add light pronation/supination work and eccentric wrist extensions; a brace can offload the tendon but doesn't fix the cause.
- Q: Should I see a physio for badminton injuries? Yes for any sharp pain, anything not resolving in 7–10 days, or anything recurrent — early care turns weeks-of-rest into days.
The four most common badminton injuries — rolled ankles, lunge-related knee strain, rotator-cuff shoulder overuse, and tennis elbow — and how to prevent each with strengthening, technique fixes and sensible training load. Practical: how to tape an ankle, when to see a physio, why over-tensioned strings cause more elbow pain than backswings, and the lunge alignment that saves knees. Not medical advice, but a player's flag for patterns that quietly end most club careers.